-
-
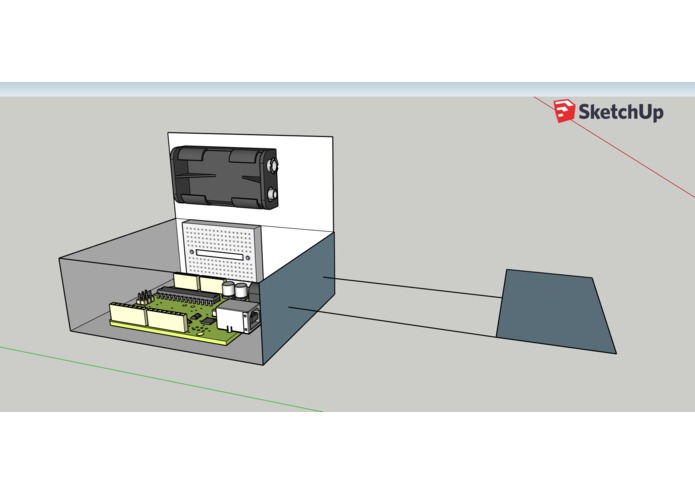
Mock up of intended prototype. Rectangle extending from unit housing represents the resistive pressure sensor.
-
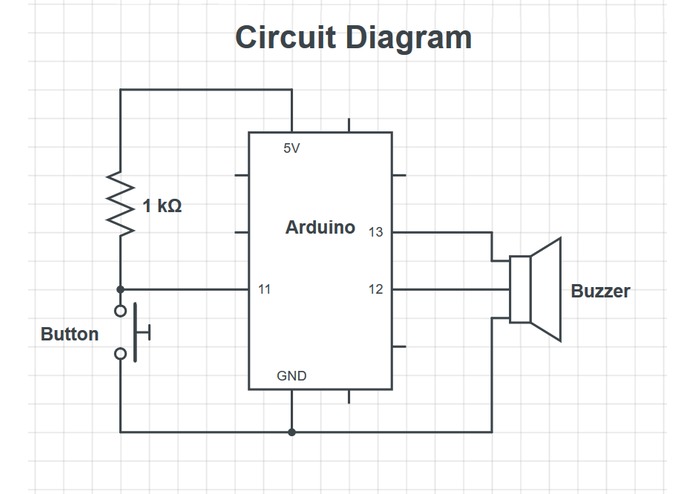
Circuit diagram of prototype


Inspiration
Falls pose a significant risk for the elderly community, resulting in approximately $30 billion in direct medical costs and severe limitations on self-reliance (Phelan et al., 2015). One method that has been introduced to facilitate fall prevention in the primary care setting is the CDC’s Stopping Elderly Accidents, Deaths, and Injuries (STEADI) toolkit, which seeks to assess and provide resources for elderly patients who are at-risk for becoming potential fall victims (Stevens and Phelan, 2013). Studies have concluded that STEADI does appear to be a useful metric for assessing a patient’s risk for fall (Lohman et al., 2017), and the patient education, self-assessment, and treatment strategies offered through the STEADI initiative can reduce fall risk by 24% (Sarmiento and Lee, 2017). Despite the benefits the STEADI program has provided in fall prevention education and assessment, specific solutions aimed at fall prevention outside the primary care setting have not been heavily marketed, aside from assistive mobility devices. In addition to the lack of product development, assistive mobility devices tend to not be adopted by the elderly community, with elderly patients citing reasons such as pride, denial of need, and embarrassment (Aminzadeh and Edwards, 1998). One avenue for potentially expanding and strengthening the STEADI initiative is providing materials and resources that physicians can recommend to patients for mitigating fall risk at home.
One risk that contributes to elderly falls is orthostatic hypotension (OH). OH occurs when patients experience a ≥ 20 mmHg drop in systolic or a ≥ 10 mmHg drop in diastolic blood pressures when they change their posture from a seated or lying position to a standing position, which can result in dizziness and potential syncope (Hiitola et al., 2009). The potential loss of consciousness not only introduces the possibility for injury but also negatively affects a patient’s self-confidence in their independence and self-care. Chronic OH can be caused by neurological and cardiac conditions, but the elderly population is vulnerable to developing OH simply through the aging process (Figueroa et al., 2010). Non-pharmaceutical methods for treating OH recommended by physicians include performing light exercises before standing, wearing compression garments, staying properly hydrated, minimizing the ingestion of OH-inducing drugs, and standing up slowly (Mills et al., 2015). While these self-treatment options provide an alternative pathway away from direct medical interventions, maintaining adherence to these practices remains a challenge (Figueroa et al., 2010). Our solution attempts to address the challenge of maintaining patient adherence to making postural transitions slowly through a sensor-based notification system. We believe that a device that assists a patient prevent OH before symptoms arise may contribute to a greater sense of independence and safety and may also contribute to a positive habit formation of making postural transitions intentionally more slowly than if they were not reminded.
What it is/ what it does
The current prototype serves as a proof of concept for the product’s viability and essential functions, but essential design upgrades and hardware changes are needed for a complete product to reach a market. A circuit diagram is included in the supplementary information section of this report. The basis of this product is an Arduino-controlled digital switch that activates the notification system of the product, which will generate a notification stimulus for the consumer. When the circuit is deactivated by the user rising from a seated position, the notification system alarms, providing a brief audio reminder to rise slowly from the seated position. The notification system is currently powered by a 5V direct-current power source. The intended application of the current prototype model is for consumers to discreetly install the product underneath toilet seats to help prevent OH-induced falls in bathrooms. Key prototype highlights include splashproof design capabilities, small device dimensions, easily managed power source, and a very simple user interface. Additional strengths of the product include the ability to specialize the device for other future applications and readily available construction materials. One potential issue with current production methods is the utilization of an Arduino-based system, which contributes significantly to the cost of production. Mass production of the product will result in reduced material costs, but initial build costs came to $21.00 per device, mainly due to the use of an Arduino microcontroller. The intended consumer price for the product is intended to be $25.00 or less. One way to address this issue is to use an alternate brand of the microcontroller.
An immediate development of this product would be to utilize an Arduino-based resistive pressure sensor to activate the notification system of the product, which will generate a notification stimulus for the consumer. When the sensor detects a change in applied pressure by the user rising from a seated position, the notification system alarms, providing a brief audio reminder to rise slowly from the seated position. The notification system is intended to be powered by a readily-available 5V direct-current battery source. The intended application of the upgraded product is to integrate it between more contact surfaces where consumers will sit. Examples include underneath toilet seats and in-between a seat cushion and a chair. Key future product highlights will include waterproof protection, reduced product size through sensor change, durable materials, and the same simple user interface as the current prototype model. Just like the current prototype, one aspect to consider for future scaleability and sustainability is the utilization of an Arduino-based system, which will contribute significantly to production costs. Mass production of the product will result in reduced construction material costs, but initial build costs came to $21.00 per unit. The cost to consumer price for the product is intended to be $25.00 or less.
Challenges we ran into
The main challenge we encountered was a lack of materials to construct the design we had in mind. We intended to use a resistive pressure sensor in the working prototype to highlight the small profile of the design, but we only had access to a digital switch. We also wanted to construct a housing unit for all the components using a 3D printer, but not having access to a 3D printer created the challenge of assembling a product without a representative housing unit. We also intended to have the unit be battery-operated, but we did not have access to a battery holder to connect to the Arduino unit.
Accomplishments that we're proud of
We are proud of assembling a working proof of concept in the time allotted, in addition to creating a fairly thorough business model and analysis of the product's usability.
What we learned
We learned that product design and engineering truly is a multidisciplinary art and science. It takes a good deal of time to think creatively for a novel solution, and it takes a lot of skill to successfully design, assemble, and test a working prototype. We also learned that solutions don't usually come overnight, but when you have unlimited access to caffeine and a team of brilliant, focused students, you can get pretty close to one in that amount of time.
What's next?
The current first step would be to optimize the product's design to include the features and housing unit we had hoped for. Constructing a marketable product is needed before approaching any market strategy. Next would be to conduct market surveys of elderly people, their families, and physicians to determine interest. Targeting physicians and family members of elderly patients as key market opportunities is the initial market strategy because those are usually the connections that encourage elderly patients to purchase assistive devices.
The current design principle is, in essence, to adjust the long-term lifestyle behaviors of the elderly, in this case helping the elderly to adjust to standing up slowly over a period of time. However, this prototype also introduces potential problems. First, the product is not targeted specifically to the human body but on shared sitting surfaces. When the seat is occupied by someone other than the targeted user, the mechanism will also be triggered creating unwanted alarm, potentially annoying the others and embarrassing the intended user. Another drawback of this design is its limited feature. Except for triggering alarms to remind the user to stand up slowly, it almost has no other use, reducing its effectiveness in a multi-feature product market.
For future product development, it’s vital to find an alternative method to detect the change of the body’s posture. Wearable devices which have a built-in gyroscope and an accelerometer can detect the motion of the limbs. Multiple devices on a single body allow for the possibility to detect and monitor complex body movements such as standing up from a chair. Moreover, wearable devices with a photoplethysmography sensor can detect heart rate and pulse oximetry. Multiple photoplethysmography sensors can detect blood pressure of the user. Such systems can target the specific user without annoying anyone else. Furthermore, an ecosystem can be implemented into the wearable devices in the form of an app, which can alarm the user when a dangerous movement occurs (e.g. standing up too quickly), let the user monitor his/her physiology continuously, and send tailored advice to the user based on his/her movement patterns. A social media feature can be further implemented to enhance the motivation of behavioral change and promote adherence to the desired routine. With the wearable device connecting to the internet, the possibility for future updates is endless.
Literature cited
Aminzadeh, F., Edwards, N., 1998. Exploring Seniors’ Views on the Use of Assistive Devices in Fall Prevention. Public Health Nurs. 15, 297–304. https://doi.org/10.1111/j.1525-1446.1998.tb00353.x Figueroa, J.J., Basford, J.R., Low, P.A., 2010. Preventing and treating orthostatic hypotension: As easy as A, B, C. Cleve. Clin. J. Med. 77, 298–306. https://doi.org/10.3949/ccjm.77a.09118 Hiitola, P., Enlund, H., Kettunen, R., Sulkava, R., Hartikainen, S., 2009. Postural changes in blood pressure and the prevalence of orthostatic hypotension among home-dwelling elderly aged 75 years or older. J. Hum. Hypertens. 23, 33–39. https://doi.org/10.1038/jhh.2008.81 Lohman, M.C., Crow, R.S., DiMilia, P.R., Nicklett, E.J., Bruce, M.L., Batsis, J.A., 2017. Operationalisation and validation of the Stopping Elderly Accidents, Deaths, and Injuries (STEADI) fall risk algorithm in a nationally representative sample. J. Epidemiol. Community Health 71, 1191–1197. https://doi.org/10.1136/jech-2017-209769 Mills, P.B., Fung, C.K., Travlos, A., Krassioukov, A., 2015. Nonpharmacologic management of orthostatic hypotension: a systematic review. Arch. Phys. Med. Rehabil. 96, 366-375.e6. https://doi.org/10.1016/j.apmr.2014.09.028 Phelan, E.A., Mahoney, J.E., Voit, J.C., Stevens, J.A., 2015. Assessment and Management of Fall Risk in Primary Care Settings. Med. Clin. North Am. 99, 281–293. https://doi.org/10.1016/j.mcna.2014.11.004 Sarmiento, K., Lee, R., 2017. STEADI: CDC’s approach to make older adult fall prevention part of every primary care practice. J. Safety Res. 63, 105–109. https://doi.org/10.1016/j.jsr.2017.08.003 Stevens, J.A., Phelan, E.A., 2013. Development of STEADI: a fall prevention resource for health care providers. Health Promot. Pract. 14, 706–714. https://doi.org/10.1177/1524839912463576
Built With
- arduino
- button-actuator
- chair
- duct-tape
- microcontroller


Log in or sign up for Devpost to join the conversation.