 When I was diagnosed with Stage four metastatic lung cancer, I pledged to launch a series of articles on tobacco, cancer, and related health issues. They won’t be in-depth, but I hope they will be thought-provoking.
When I was diagnosed with Stage four metastatic lung cancer, I pledged to launch a series of articles on tobacco, cancer, and related health issues. They won’t be in-depth, but I hope they will be thought-provoking. killer. History records that his “Great Leap Forward” movement, killed 45 million of his own people in just four years. Again, though, the numbers are so great they are meaningless statistics. The human mind can visualize 10, 20, or even 100 bodies, but 45 million dead bodies? Hardly, so the number has little or no visual effect.
killer. History records that his “Great Leap Forward” movement, killed 45 million of his own people in just four years. Again, though, the numbers are so great they are meaningless statistics. The human mind can visualize 10, 20, or even 100 bodies, but 45 million dead bodies? Hardly, so the number has little or no visual effect. The deaths caused by Stalin and Mao pale, though, when compared to the numbers piled up by the likes of Pierre Lorillard, Richard Joshua Reynolds, Phillip Morris and others whose tobacco companies are collectively responsible for the deaths of up to a hundred million people in the 20th century. That toll, according to WHO (the World Health Organization) is on track to kill over one billion people in the 21st century.
The deaths caused by Stalin and Mao pale, though, when compared to the numbers piled up by the likes of Pierre Lorillard, Richard Joshua Reynolds, Phillip Morris and others whose tobacco companies are collectively responsible for the deaths of up to a hundred million people in the 20th century. That toll, according to WHO (the World Health Organization) is on track to kill over one billion people in the 21st century. had a murder for money scheme. They persuaded their victims to purchase the poison that killed them. When I smoked, cigarettes were fairly inexpensive. Still, I calculate averaging 35 cents a pack and smoking 3 to 4 packs a day; I paid R. J. Reynolds some $20,000 to kill me. “Winston’s taste good like a cigarette should,” worked on me. Today at $6.00 or more a pack tobacco profits are even higher.
had a murder for money scheme. They persuaded their victims to purchase the poison that killed them. When I smoked, cigarettes were fairly inexpensive. Still, I calculate averaging 35 cents a pack and smoking 3 to 4 packs a day; I paid R. J. Reynolds some $20,000 to kill me. “Winston’s taste good like a cigarette should,” worked on me. Today at $6.00 or more a pack tobacco profits are even higher. A hundred million, dead. A billion dead. Who can even begin to comprehend that number of bodies? No one! And the tobacco companies counted on it. I’m sure I’ll be tossed into the statistical “forgotten” heap, too, but maybe one or two of my blogs and those of my “Statistical” colleagues will survive to indicate that we were human beings, that we had some value and deserved better. We are not statistics. We are not digital data points; we are people who lived, loved, and added value to our communities. You cannot silence us by diminishing our importance. Your ashtray of statistics will continue to be exposed as a murderous cover-up, as our chorus of protests overwhelms your statistical graves.
A hundred million, dead. A billion dead. Who can even begin to comprehend that number of bodies? No one! And the tobacco companies counted on it. I’m sure I’ll be tossed into the statistical “forgotten” heap, too, but maybe one or two of my blogs and those of my “Statistical” colleagues will survive to indicate that we were human beings, that we had some value and deserved better. We are not statistics. We are not digital data points; we are people who lived, loved, and added value to our communities. You cannot silence us by diminishing our importance. Your ashtray of statistics will continue to be exposed as a murderous cover-up, as our chorus of protests overwhelms your statistical graves. dying from tobacco use; I feel compelled to try again to offer an example of the carnage. The Airbus A-380 that can carry 555 or more passengers is the largest airplane in the world. If two of them crashed every day for a year, and human bodies and body parts covered the crash sites, the toll would equal the number killed by tobacco in a year, and the media would be filled with gory pictures of the crash sites. Politicians voices would dominate the airwaves demanding investigations, newspapers would publish lengthy reports, airline executives would be arrested and jailed, and Airbus would cease to exist.
dying from tobacco use; I feel compelled to try again to offer an example of the carnage. The Airbus A-380 that can carry 555 or more passengers is the largest airplane in the world. If two of them crashed every day for a year, and human bodies and body parts covered the crash sites, the toll would equal the number killed by tobacco in a year, and the media would be filled with gory pictures of the crash sites. Politicians voices would dominate the airwaves demanding investigations, newspapers would publish lengthy reports, airline executives would be arrested and jailed, and Airbus would cease to exist. Still, an equal number of people die from smoking and there is no outrage, there are no protests or investigations and no one, not a single tobacco executive is behind bars. Why? Why is my death less important because of the way I died? Why am I a statistic and the others are real people whose pictures dominate the front pages of the world? Why is that? It’s because Stalin’s hypothesis is true. I and others like me are cast into that pile of unbelievable, unimaginable statistics because we die quietly without fanfare and gory
Still, an equal number of people die from smoking and there is no outrage, there are no protests or investigations and no one, not a single tobacco executive is behind bars. Why? Why is my death less important because of the way I died? Why am I a statistic and the others are real people whose pictures dominate the front pages of the world? Why is that? It’s because Stalin’s hypothesis is true. I and others like me are cast into that pile of unbelievable, unimaginable statistics because we die quietly without fanfare and gory  pictures. We died not in fiery crashes but rather coughing, and in pain, one at a time rather than in large groups.
pictures. We died not in fiery crashes but rather coughing, and in pain, one at a time rather than in large groups. s also a cancer victim. His son, Michael O’Meara had later said:
s also a cancer victim. His son, Michael O’Meara had later said: justice but, R.J. Reynolds Senior, the founder of the company that makes Winston, Camels and other tobacco brands, died of pancreatic cancer, which is tied to tobacco use.
justice but, R.J. Reynolds Senior, the founder of the company that makes Winston, Camels and other tobacco brands, died of pancreatic cancer, which is tied to tobacco use. Communications Consultant, Bob Aronson smoked for 37 years. He quit the habit nearly 30 years ago after developing COPD (Chronic Obstructive Pulmonary Disease). A failing heart, probably caused by smoking, resulted in his receiving a heart transplant in 2007. In June of 2018, he was diagnosed with Stage Four Metastatic Lung Cancer, likely caused by his smoking combined with a compromised immune system due to his need for anti-rejection drugs to protect his transplanted heart. He is currently being treated at the Mayo Clinic in Jacksonville, Florida where he lives with his wife Robin and their dogs Reilly and Ziggy.
Communications Consultant, Bob Aronson smoked for 37 years. He quit the habit nearly 30 years ago after developing COPD (Chronic Obstructive Pulmonary Disease). A failing heart, probably caused by smoking, resulted in his receiving a heart transplant in 2007. In June of 2018, he was diagnosed with Stage Four Metastatic Lung Cancer, likely caused by his smoking combined with a compromised immune system due to his need for anti-rejection drugs to protect his transplanted heart. He is currently being treated at the Mayo Clinic in Jacksonville, Florida where he lives with his wife Robin and their dogs Reilly and Ziggy. Yes, there is an opioid crisis. Yes, the number of deaths from opioid overdoses is a tragedy, and yes, something must be done to stop the addiction and the dying, but denying pain relief to legitimate chronic pain sufferers is not the way to do it. There are millions of Americans who suffer daily from chronic pain and need the relief provided by opioids. Everyone is subject to becoming a chronic pain sufferer including transplant recipients.
Yes, there is an opioid crisis. Yes, the number of deaths from opioid overdoses is a tragedy, and yes, something must be done to stop the addiction and the dying, but denying pain relief to legitimate chronic pain sufferers is not the way to do it. There are millions of Americans who suffer daily from chronic pain and need the relief provided by opioids. Everyone is subject to becoming a chronic pain sufferer including transplant recipients. 2018, CMS (Centers for Medicare and Medicaid Services) issued updated regulations for Medicare Advantage Plans (MAP) and Medicare Part D programs. The focus of the updates is to provide additional guidelines and tools to target the nation’s growing opioid epidemic. I should note that most, perhaps 90 percent of those affected are older Americans. The Government has targeted chronic pain patients many of whom are senior citizens. Here’s proof. CDC’s Guideline for Prescribing Opioids for chronic pain makes it clear that pain patients should be using alternative therapies that do not include narcotics regardless of the level of pain and effectiveness of the alternative treatment. The Guidelines ignore the fact that many patients cannot afford alternatives, are disabled and unable to get to alternative therapy and that many are uninsured and cannot afford it.
2018, CMS (Centers for Medicare and Medicaid Services) issued updated regulations for Medicare Advantage Plans (MAP) and Medicare Part D programs. The focus of the updates is to provide additional guidelines and tools to target the nation’s growing opioid epidemic. I should note that most, perhaps 90 percent of those affected are older Americans. The Government has targeted chronic pain patients many of whom are senior citizens. Here’s proof. CDC’s Guideline for Prescribing Opioids for chronic pain makes it clear that pain patients should be using alternative therapies that do not include narcotics regardless of the level of pain and effectiveness of the alternative treatment. The Guidelines ignore the fact that many patients cannot afford alternatives, are disabled and unable to get to alternative therapy and that many are uninsured and cannot afford it.  Always remember, these are
Always remember, these are  pain-relieving drugs will strengthen their bottom line, they will do it. This war on opioids then becomes a profit center for Part D. Insurance companies. CMS (Centers for Medicare and Medicaid Services) says it will designate all opioids, except Buprenorphine (a drug used to treat opioid dependence) and Benzodiazepines (an addictive drug used to treat anxiety, nervousness, panic disorders, muscle spasms, seizures, and more). Benzos will also be designated as a frequently abused drugs but will be excluded from the new guidelines, for a while). You can read more here — CMS proposes Part D Opioid Limits, Pharmacy reacts.
pain-relieving drugs will strengthen their bottom line, they will do it. This war on opioids then becomes a profit center for Part D. Insurance companies. CMS (Centers for Medicare and Medicaid Services) says it will designate all opioids, except Buprenorphine (a drug used to treat opioid dependence) and Benzodiazepines (an addictive drug used to treat anxiety, nervousness, panic disorders, muscle spasms, seizures, and more). Benzos will also be designated as a frequently abused drugs but will be excluded from the new guidelines, for a while). You can read more here — CMS proposes Part D Opioid Limits, Pharmacy reacts. 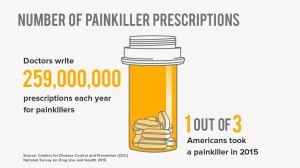 Administration), the FDA (Food and Drug Administration) and the CDC (Centers for Disease Control). CDC reports that opioids were involved in 42,249 deaths in 2016, and opioid overdose deaths were five times higher in 2016 than 1 999.
Administration), the FDA (Food and Drug Administration) and the CDC (Centers for Disease Control). CDC reports that opioids were involved in 42,249 deaths in 2016, and opioid overdose deaths were five times higher in 2016 than 1 999. make opioids, 2) the physicians who prescribe them, 3) the pharmacies that fill the prescriptions and 4) the patients who need them. CDC says that each year,
make opioids, 2) the physicians who prescribe them, 3) the pharmacies that fill the prescriptions and 4) the patients who need them. CDC says that each year,  watching you and want you to know that we strongly discourage prescribing opioids for repeat patients. If you continue to do that you are placing your license at risk.”” So, who is a repeat patient? That’s me and thousands if not millions like me who must see a physician each month to get a new opioid prescription. There is far less pressure on docs who write a scrip for one or two-time use. That’s someone who broke an arm, and in a few weeks, the pain is gone on its own as opposed to Chronic Pain patients who need on-going relief.
watching you and want you to know that we strongly discourage prescribing opioids for repeat patients. If you continue to do that you are placing your license at risk.”” So, who is a repeat patient? That’s me and thousands if not millions like me who must see a physician each month to get a new opioid prescription. There is far less pressure on docs who write a scrip for one or two-time use. That’s someone who broke an arm, and in a few weeks, the pain is gone on its own as opposed to Chronic Pain patients who need on-going relief. Recently on Facebook I posted some thoughts on the opioid crisis. It got a lot of reaction. The opioid crisis of which I speak is not the one that’s in the news every day. This one rarely gets any news coverage.
Recently on Facebook I posted some thoughts on the opioid crisis. It got a lot of reaction. The opioid crisis of which I speak is not the one that’s in the news every day. This one rarely gets any news coverage. called “pill mills” are shut down and physicians and others are rounded up as an epidemic about to sweep away the foundations of our society. In a wild, irrational state of panic they spread ignorance and lies that would have everyone believe that millions are getting painkillers they don’t need from crooked physicians and then selling them on the streets or overdosing.
called “pill mills” are shut down and physicians and others are rounded up as an epidemic about to sweep away the foundations of our society. In a wild, irrational state of panic they spread ignorance and lies that would have everyone believe that millions are getting painkillers they don’t need from crooked physicians and then selling them on the streets or overdosing. That’s not to say there isn’t some truth to their crisis claims, but to attempt to shut down narcotics prescriptions all over America is an overreaction that is already generating horrific consequences. This reaction is not dissimilar to the often heard claim that most welfare recipients are cheats and therefore we have to cut welfare programs to the core and beyond.
That’s not to say there isn’t some truth to their crisis claims, but to attempt to shut down narcotics prescriptions all over America is an overreaction that is already generating horrific consequences. This reaction is not dissimilar to the often heard claim that most welfare recipients are cheats and therefore we have to cut welfare programs to the core and beyond. What is ignored in this crackdown on opioids is that there are thousands and thousands of people who suffer with chronic pain. I’m one of them, my brother is another and I know many more as well. This overreaction to a problem is causing suffering beyond belief. If you’ve never experienced the kind of pain that has you on your knees, crying and begging for relief, then you have no business judging those who are in that situation. If you’ve never had or seen pain so bad, you pray for a quick death then you have no right to suggest policy. If everything you know about drug abuse comes from talk shows and the internet, you have no right to attempt to interfere in the lives of those who live with it every day.
What is ignored in this crackdown on opioids is that there are thousands and thousands of people who suffer with chronic pain. I’m one of them, my brother is another and I know many more as well. This overreaction to a problem is causing suffering beyond belief. If you’ve never experienced the kind of pain that has you on your knees, crying and begging for relief, then you have no business judging those who are in that situation. If you’ve never had or seen pain so bad, you pray for a quick death then you have no right to suggest policy. If everything you know about drug abuse comes from talk shows and the internet, you have no right to attempt to interfere in the lives of those who live with it every day. result is that many physicians just plain refuse to write narcotics prescriptions. There are major healthcare organizations that have adopted the same policy. Most cruel, though, is the action taken by many reputable pain clinics to offer narcotic-free pain relief. Nice claim, but Impossible. No I’m not a doctor but I have intense pain and I know what provides relief and what doesn’t.
result is that many physicians just plain refuse to write narcotics prescriptions. There are major healthcare organizations that have adopted the same policy. Most cruel, though, is the action taken by many reputable pain clinics to offer narcotic-free pain relief. Nice claim, but Impossible. No I’m not a doctor but I have intense pain and I know what provides relief and what doesn’t. We don’t live in a black and white world. There are many shades of gray. This paranoia about narcotics is the same as the ignorance that suggests that anyone who takes narcotics will be addicted, or any physician who prescribes them is a greedy criminal. It is the same as believing all welfare recipients are cheating the system and immigrants are inherently dangerous. This incredibly narrow minded approach to any problem is the result of a nation that no longer honors education, refuses to read, gets its information from talk shows and rarely thinks beyond the latest talk show or political one-liner. We have become a nation that believes in junk science, junk history, junk education, junk leaders and junk wisdom. You might be happy with that simple approach to life until you find yourself in need of food, heaalthcare, or compassion. I hope that real wisdom strikes our nation before any of the true-believers in that black and white world develop a condition that causes them unbearable physical pain for which no one will provide relief.
We don’t live in a black and white world. There are many shades of gray. This paranoia about narcotics is the same as the ignorance that suggests that anyone who takes narcotics will be addicted, or any physician who prescribes them is a greedy criminal. It is the same as believing all welfare recipients are cheating the system and immigrants are inherently dangerous. This incredibly narrow minded approach to any problem is the result of a nation that no longer honors education, refuses to read, gets its information from talk shows and rarely thinks beyond the latest talk show or political one-liner. We have become a nation that believes in junk science, junk history, junk education, junk leaders and junk wisdom. You might be happy with that simple approach to life until you find yourself in need of food, heaalthcare, or compassion. I hope that real wisdom strikes our nation before any of the true-believers in that black and white world develop a condition that causes them unbearable physical pain for which no one will provide relief. we diminish our history, our potential and everything for which our founders stood. A mood of selfishness and unreasonable approaches to law and order has grown deep roots in America. Only when we have restored our moral and ethical compass will we stand a chance of emerging as the thought and compassion leader we like to believe we are.
we diminish our history, our potential and everything for which our founders stood. A mood of selfishness and unreasonable approaches to law and order has grown deep roots in America. Only when we have restored our moral and ethical compass will we stand a chance of emerging as the thought and compassion leader we like to believe we are.
 If you have difficulty getting around for any reason a mobility scooter may be in your future but before you run out and buy one, you should read this. It should answer most of your questions and if not it will provide links to sites that can be helpful. This is a serious effort to respond to questions based on my own experience of purchasing three mobility scooters over the past five years for my own use.
If you have difficulty getting around for any reason a mobility scooter may be in your future but before you run out and buy one, you should read this. It should answer most of your questions and if not it will provide links to sites that can be helpful. This is a serious effort to respond to questions based on my own experience of purchasing three mobility scooters over the past five years for my own use. compare them to mobility scooters, they are totally different because they are a single purpose vehicle. They are built to stay indoors, carry a lot of weight, turn around in an aisle and move slower than a glacier. All of those qualities are great for a supermarket but serve little purpose at home or for outdoor travel.
compare them to mobility scooters, they are totally different because they are a single purpose vehicle. They are built to stay indoors, carry a lot of weight, turn around in an aisle and move slower than a glacier. All of those qualities are great for a supermarket but serve little purpose at home or for outdoor travel. can make that determination. If you are seeking government financial help for mobility assistance your physician will first have to formally make that declaration. He or she will use certain conditions to determine if you qualify. Most physicians use the criteria established by Medicare and Medicare Part B. Included in these conditions, as outlined on the Medicare website, are:
can make that determination. If you are seeking government financial help for mobility assistance your physician will first have to formally make that declaration. He or she will use certain conditions to determine if you qualify. Most physicians use the criteria established by Medicare and Medicare Part B. Included in these conditions, as outlined on the Medicare website, are:

 Spitfire Scout, require no added expense because it can be disassembled and tossed in your trunk quite easily often by the user him or herself (you can purchase a rear bumper platform that will elevate and secure the scooter for outside your car or van transportation but these can be costly)..
Spitfire Scout, require no added expense because it can be disassembled and tossed in your trunk quite easily often by the user him or herself (you can purchase a rear bumper platform that will elevate and secure the scooter for outside your car or van transportation but these can be costly).. with access through the side door. A folding aluminum ramp cost about $200, a remote controlled winch was another $100 and we used one of those jump-start batteries to power the winch which cost another $100. The rest is easy. I drive the scooter to the edge of the ramp, connect the winch hook to the frame of the scooter and with a flick of a switch on the remote control, pull the scooter into the van. The whole process from setting up the ramp to securing the scooter inside takes about 5 minutes.
with access through the side door. A folding aluminum ramp cost about $200, a remote controlled winch was another $100 and we used one of those jump-start batteries to power the winch which cost another $100. The rest is easy. I drive the scooter to the edge of the ramp, connect the winch hook to the frame of the scooter and with a flick of a switch on the remote control, pull the scooter into the van. The whole process from setting up the ramp to securing the scooter inside takes about 5 minutes. If you approach a bump or curb at an angle instead of head-on you run the risk of tipping. Finding yourself on your side on a sidewalk, a berm or in the street with your groceries rolling around is not a comfortable feeling. When I tipped it was when crossing a street probably due to my driving error. A scooter doesn’t respond like a car or resemble the family auto in any way. If driven properly they are quite safe, but if you violate the instructions you could be seriously injured. When climbing a curb or going over an elevation in the ground the driver must be careful to follow the instructions in the owner’s manual. Most people ignore the instructions or warnings in a manual. Don’t! Read them a couple of times.
If you approach a bump or curb at an angle instead of head-on you run the risk of tipping. Finding yourself on your side on a sidewalk, a berm or in the street with your groceries rolling around is not a comfortable feeling. When I tipped it was when crossing a street probably due to my driving error. A scooter doesn’t respond like a car or resemble the family auto in any way. If driven properly they are quite safe, but if you violate the instructions you could be seriously injured. When climbing a curb or going over an elevation in the ground the driver must be careful to follow the instructions in the owner’s manual. Most people ignore the instructions or warnings in a manual. Don’t! Read them a couple of times. An often overlooked item is a ramp. If you keep your scooter in the house and want to take it out the front door, even if it is at ground level you may need a small ramp to keep from getting hung up on the threshold. If you are going to do that often, please consider having a ramp built according to the disability codes in your city. If you rarely go out, a small folding aluminum ramp could be a great help. The weight of a ramp, though, depends on how long it is and the ADA (Americans with Disabilities Act) has requirements for how long a ramp should be. This link will help you determine the proper size for your needs.
An often overlooked item is a ramp. If you keep your scooter in the house and want to take it out the front door, even if it is at ground level you may need a small ramp to keep from getting hung up on the threshold. If you are going to do that often, please consider having a ramp built according to the disability codes in your city. If you rarely go out, a small folding aluminum ramp could be a great help. The weight of a ramp, though, depends on how long it is and the ADA (Americans with Disabilities Act) has requirements for how long a ramp should be. This link will help you determine the proper size for your needs.  at night in the dark. Even if you think you will never have to take your scooter outside, I can assure you that at some point that’s where you will find yourself. For example, we have dogs. Dogs need to be walked. I have difficulty walking so I learned to take them for a “scooter walk.” If you have an indoors scooter it likely will have minimal ground clearance. You may need the lights to see the uneven ground ahead of you to avoid damaging your scooter or, worse yet, tipping and hurting yourself. Scooters, even the big ones, are hard to see so if you decide to purchase a bare bones, no lighting scooter, go to Wal*Mart or Target and purchase a headlight, a taillight and some
at night in the dark. Even if you think you will never have to take your scooter outside, I can assure you that at some point that’s where you will find yourself. For example, we have dogs. Dogs need to be walked. I have difficulty walking so I learned to take them for a “scooter walk.” If you have an indoors scooter it likely will have minimal ground clearance. You may need the lights to see the uneven ground ahead of you to avoid damaging your scooter or, worse yet, tipping and hurting yourself. Scooters, even the big ones, are hard to see so if you decide to purchase a bare bones, no lighting scooter, go to Wal*Mart or Target and purchase a headlight, a taillight and some  reflectors for the back and sides. You should be able to get all three for under $20 at the stores mentioned, at any bicycle supply dealer or from any of the on-line sellers like Amazon and EBay. All scooters are very close to the ground and it pays to be lit up like a Christmas tree along with having one of those bicycle or scooter safety flags on the back. I don’t recommend driving your scooter on the street but sometimes it is unavoidable….that means you should also have a rear view mirror and even a horn. You need to be totally aware of your surroundings and you need to let your surroundings know you are there.
reflectors for the back and sides. You should be able to get all three for under $20 at the stores mentioned, at any bicycle supply dealer or from any of the on-line sellers like Amazon and EBay. All scooters are very close to the ground and it pays to be lit up like a Christmas tree along with having one of those bicycle or scooter safety flags on the back. I don’t recommend driving your scooter on the street but sometimes it is unavoidable….that means you should also have a rear view mirror and even a horn. You need to be totally aware of your surroundings and you need to let your surroundings know you are there. is important. That’s especially true of the larger scooters that have four-wheel suspension (springs) where the shock of hitting a bump is dampened before it gets to your rump. The air-filled tires help absorb some of the shock. Smaller scooters don’t have suspension of any kind so they ride like a skate board anyway. Most of them don’t come with pneumatic tires. There are circumstances where tires become extremely important and that is almost always outside of the home. Bigger, wider, tougher tires are a necessity if you are traveling over rough terrain, near construction sites, in sand or grass or a number of other situations. Thin, small tires likely will get stuck very quickly in adverse conditions. Scooters for use out of doors should always have tires that are at least 10 or 12 inches in diameter and 3 inches wide (the Panther’s tires are 14 X 4)
is important. That’s especially true of the larger scooters that have four-wheel suspension (springs) where the shock of hitting a bump is dampened before it gets to your rump. The air-filled tires help absorb some of the shock. Smaller scooters don’t have suspension of any kind so they ride like a skate board anyway. Most of them don’t come with pneumatic tires. There are circumstances where tires become extremely important and that is almost always outside of the home. Bigger, wider, tougher tires are a necessity if you are traveling over rough terrain, near construction sites, in sand or grass or a number of other situations. Thin, small tires likely will get stuck very quickly in adverse conditions. Scooters for use out of doors should always have tires that are at least 10 or 12 inches in diameter and 3 inches wide (the Panther’s tires are 14 X 4) Well, kind of. I’m not sure if all manufacturers use the same criteria for making that determination but how far you can go depends entirely on how much weight the scooter is carrying, how fast you are going and if the battery was fully charged when you left. The fact is I rarely ever even consider the range because most of my trips are short and I put the scooter on the charger when I return from my journey. In five years of riding scooters I have never even come close to running out of power.
Well, kind of. I’m not sure if all manufacturers use the same criteria for making that determination but how far you can go depends entirely on how much weight the scooter is carrying, how fast you are going and if the battery was fully charged when you left. The fact is I rarely ever even consider the range because most of my trips are short and I put the scooter on the charger when I return from my journey. In five years of riding scooters I have never even come close to running out of power. not designed or built to be recreational vehicles either. They are designed to help disabled persons get from point A to point B. A mobility scooter is not a toy but it is also not a car or bus. You can have the most decked-out, high-priced scooter ever made and it still won’t perform like a car or an ATV. Your 150 lb. scooter traveling at 7 miles an hour is no match for a 3500 lb. car going 45 or 50. Remember that if you think about getting off the sidewalk and onto the street. Be cautious, responsible and extremely careful. Keep in mind that you have a scooter and it should be ridden on sidewalks and paved areas. Avoid riding on streets. Even the fastest of scooters will only go 15 miles an hour, far too slow to stay with traffic and far too small to be seen. However, if construction or other barriers force you to get into the flow of traffic on a street and your scooter has a lighting package turn on your flashers, put up a safety flag and look for a place to get back on the sidewalk as fast as possible.
not designed or built to be recreational vehicles either. They are designed to help disabled persons get from point A to point B. A mobility scooter is not a toy but it is also not a car or bus. You can have the most decked-out, high-priced scooter ever made and it still won’t perform like a car or an ATV. Your 150 lb. scooter traveling at 7 miles an hour is no match for a 3500 lb. car going 45 or 50. Remember that if you think about getting off the sidewalk and onto the street. Be cautious, responsible and extremely careful. Keep in mind that you have a scooter and it should be ridden on sidewalks and paved areas. Avoid riding on streets. Even the fastest of scooters will only go 15 miles an hour, far too slow to stay with traffic and far too small to be seen. However, if construction or other barriers force you to get into the flow of traffic on a street and your scooter has a lighting package turn on your flashers, put up a safety flag and look for a place to get back on the sidewalk as fast as possible.
 it. They have made many claims about what a “Disaster” it is, but offer little in the way of evidence other than point to increased premiums. Premiums, though, were out of control long before there was an ACA and many experts say that if anything the sweeping health care bill slowed their increase. If Republicans are successful in repealing the act you will be affected in many ways, now and in the future. I’d like to keep this blog relatively short so I will only address four issues here, but they are big ones.
it. They have made many claims about what a “Disaster” it is, but offer little in the way of evidence other than point to increased premiums. Premiums, though, were out of control long before there was an ACA and many experts say that if anything the sweeping health care bill slowed their increase. If Republicans are successful in repealing the act you will be affected in many ways, now and in the future. I’d like to keep this blog relatively short so I will only address four issues here, but they are big ones. If the ACA is repealed without a replacement plan and maybe even with one here’s what you can expect.
If the ACA is repealed without a replacement plan and maybe even with one here’s what you can expect. once you turn 19 or are no longer a full-time student, you are on your own for insurance coverage, increasing the financial burden on young adults who are unemployed, underemployed, contractors, working for small companies, or those starting their own businesses. Young people are less likely to get seriously ill and often don’t use insurance when they have it. Insurance companies would love to have these men and women paying premiums again, though, because they use so little of the coverage and help to defray the cost of covering others.
once you turn 19 or are no longer a full-time student, you are on your own for insurance coverage, increasing the financial burden on young adults who are unemployed, underemployed, contractors, working for small companies, or those starting their own businesses. Young people are less likely to get seriously ill and often don’t use insurance when they have it. Insurance companies would love to have these men and women paying premiums again, though, because they use so little of the coverage and help to defray the cost of covering others. News
News services performed under the managed-care portion of Medicare known as Medicare Advantage. That, then, could lead to increased Medicare Advantage premiums. It could also mean an end to free preventive services and could result in greater premiums and increased out-of-pocket costs, or both.
services performed under the managed-care portion of Medicare known as Medicare Advantage. That, then, could lead to increased Medicare Advantage premiums. It could also mean an end to free preventive services and could result in greater premiums and increased out-of-pocket costs, or both. Bob Aronson is the founder of Facebook’s 4300 member Organ Transplant Initiative and also of this site, Bob’s Newheart. Look through the index and you’ll find nearly 300 blogs of interest to Transplant patients, their families, friends, caregivers, donors and donor families.
Bob Aronson is the founder of Facebook’s 4300 member Organ Transplant Initiative and also of this site, Bob’s Newheart. Look through the index and you’ll find nearly 300 blogs of interest to Transplant patients, their families, friends, caregivers, donors and donor families.  The time had come. Claire Connelly was finally going to meet the man who had her son Paul’s heart. She would travel from southern to northern California by train to meet him. This trip was more than just an opportunity to meet the man, it was the culmination of a three-year long search. Claire was determined to let nothi
The time had come. Claire Connelly was finally going to meet the man who had her son Paul’s heart. She would travel from southern to northern California by train to meet him. This trip was more than just an opportunity to meet the man, it was the culmination of a three-year long search. Claire was determined to let nothi ng get in the way of this meeting. She was so afraid that she might oversleep and miss her train, she drove to the Amtrak station the evening before and slept in her van in the parking lot. Meeting her son’s’ heart recipient had become Claire’s sole purpose in life, so when she boarded that train last Monday morning her heart was in her throat.
ng get in the way of this meeting. She was so afraid that she might oversleep and miss her train, she drove to the Amtrak station the evening before and slept in her van in the parking lot. Meeting her son’s’ heart recipient had become Claire’s sole purpose in life, so when she boarded that train last Monday morning her heart was in her throat. I wrote about her in a blog on October 21, 2016. To meet her, even by phone is to love her. She is kind, upbeat, considerate and passionate about life and living. Claire is your favorite aunt — you know, the one who is funny, always has a gift for you and really listens to what you have to say. She’s one of those people who brings energy and love of life into any conversation. When you talk; with Claire you can’t help but feel good.
I wrote about her in a blog on October 21, 2016. To meet her, even by phone is to love her. She is kind, upbeat, considerate and passionate about life and living. Claire is your favorite aunt — you know, the one who is funny, always has a gift for you and really listens to what you have to say. She’s one of those people who brings energy and love of life into any conversation. When you talk; with Claire you can’t help but feel good.
 the same date on the calendar?”
the same date on the calendar?” of random thoughts that somehow merged like two sets of railroad tracks. Claire kept a journal as the train sped north. If you close your eyes you can almost hear the clacking of the wheels on the track and the whistle being blown as intersections are crossed.
of random thoughts that somehow merged like two sets of railroad tracks. Claire kept a journal as the train sped north. If you close your eyes you can almost hear the clacking of the wheels on the track and the whistle being blown as intersections are crossed. make one thing very clear, this is not my story or Ken’s. My son Paul is the hero here. Long ago he made the decision to become an organ donor. All I did was to ensure that his wishes were fulfilled.
make one thing very clear, this is not my story or Ken’s. My son Paul is the hero here. Long ago he made the decision to become an organ donor. All I did was to ensure that his wishes were fulfilled. 



 Bob Aronson is a 2007 heart transplant recipient and the founder of this blog which contains nearly 300 posts on donation/transplantation and associated issues. If you need a support group, please join Facebook’s Organ Transplant Initiative. And if you are not yet an organ donor, sign up now, it takes almost none of your time and you can do it from where you are sitting. Log on to
Bob Aronson is a 2007 heart transplant recipient and the founder of this blog which contains nearly 300 posts on donation/transplantation and associated issues. If you need a support group, please join Facebook’s Organ Transplant Initiative. And if you are not yet an organ donor, sign up now, it takes almost none of your time and you can do it from where you are sitting. Log on to  Over the years I’ve written a great deal about organ donation and whether we should continue with the altruistic program we have now, or consider some sort of compensation for organ donors and/or families.
Over the years I’ve written a great deal about organ donation and whether we should continue with the altruistic program we have now, or consider some sort of compensation for organ donors and/or families. over 30 years ago keeps falling farther and farther behind the demand, then I cannot help but think the system is failing. The system is not a total failure because it does save many lives, but it is failing because the gap between supply and demand is widening. Now I suspect that some people will argue the “Failing” point, but you can’t argue with the numbers. The system isn’t working. And every time new approaches are proposed, like some sort of compensation, the ethicists loudly proclaim that the practice would be unethical. Ok, but what’s ethical about allowing 8,000 people to die each year because there are not enough organs? Why isn’t someone questioning the ethics of that fact?
over 30 years ago keeps falling farther and farther behind the demand, then I cannot help but think the system is failing. The system is not a total failure because it does save many lives, but it is failing because the gap between supply and demand is widening. Now I suspect that some people will argue the “Failing” point, but you can’t argue with the numbers. The system isn’t working. And every time new approaches are proposed, like some sort of compensation, the ethicists loudly proclaim that the practice would be unethical. Ok, but what’s ethical about allowing 8,000 people to die each year because there are not enough organs? Why isn’t someone questioning the ethics of that fact? Before we get into what can be done about the organ shortage we should discuss briefly the two kinds of organ donors. There are living donors, people who can donate one of their two kidneys or a part of a liver. And – there are deceased donors. In both cases insurance will pay for the removal and transplantation of the organs, it costs the donor absolutely nothing. But there are other expenses that are not paid.
Before we get into what can be done about the organ shortage we should discuss briefly the two kinds of organ donors. There are living donors, people who can donate one of their two kidneys or a part of a liver. And – there are deceased donors. In both cases insurance will pay for the removal and transplantation of the organs, it costs the donor absolutely nothing. But there are other expenses that are not paid. Here’s an example. In 1993 a man later identified as William Michael Lucas, 34, an unemployed man was badly beaten outside his home. He was taken to the hospital and treated, but finally after an extended and expensive hospital stay, succumbed to his massive injuries. It was determined that some of his organs were transplantable and his heart and liver went to Pennsylvania Governor Robert Casey.
Here’s an example. In 1993 a man later identified as William Michael Lucas, 34, an unemployed man was badly beaten outside his home. He was taken to the hospital and treated, but finally after an extended and expensive hospital stay, succumbed to his massive injuries. It was determined that some of his organs were transplantable and his heart and liver went to Pennsylvania Governor Robert Casey. I want to be perfectly clear here, I have no problem with those mentioned getting paid, they are all people and organizations with very special skills and they deserve to be compensated. But didn’t the Lucas family deserve some consideration. Wouldn’t it make just a little bit of sense to relieve them of the medical bills and the funeral burden and maybe some grief counseling, too? That seems only fair.
I want to be perfectly clear here, I have no problem with those mentioned getting paid, they are all people and organizations with very special skills and they deserve to be compensated. But didn’t the Lucas family deserve some consideration. Wouldn’t it make just a little bit of sense to relieve them of the medical bills and the funeral burden and maybe some grief counseling, too? That seems only fair. This policy makes absolutely no sense because, ironically, Medicare will pay for a lifetime of dialysis if you go into rejection because you can’t afford to buy the drugs that prevent it, Medicare will even pay for another transplant and/or dialysis at costs that are many times the annual expense of immunosuppressant drugs. This political sleight of hand act not only wastes U.S. taxpayer dollars, it can actually cause death.
This policy makes absolutely no sense because, ironically, Medicare will pay for a lifetime of dialysis if you go into rejection because you can’t afford to buy the drugs that prevent it, Medicare will even pay for another transplant and/or dialysis at costs that are many times the annual expense of immunosuppressant drugs. This political sleight of hand act not only wastes U.S. taxpayer dollars, it can actually cause death. in the United States. The only nation in the world that allows for it is Iran and Iran, as a result, has no organ shortage. In Iran Two charities facilitate the process by finding potential vendors and introducing them to the recipients, and are charged with checking the compatibility of a possible donation and ensuring a fair trade. After the transplant, the vendor is compensated by both the government and the recipient. Iranians are not allowed to donate kidneys to non-citizens. In the U.S. the argument against paying people for their organs (living donors of kidneys and livers) is that the practice would prey on the poor. Supposedly only people who are in desperate need of money would sell their organs. “The rich or reasonably well off,” the argument goes, “Don’t need the money so few of them would become donors under such a system.” Additionally, wealthy people could buy organs from the poor but the poor could not afford to buy organs if they needed them.
in the United States. The only nation in the world that allows for it is Iran and Iran, as a result, has no organ shortage. In Iran Two charities facilitate the process by finding potential vendors and introducing them to the recipients, and are charged with checking the compatibility of a possible donation and ensuring a fair trade. After the transplant, the vendor is compensated by both the government and the recipient. Iranians are not allowed to donate kidneys to non-citizens. In the U.S. the argument against paying people for their organs (living donors of kidneys and livers) is that the practice would prey on the poor. Supposedly only people who are in desperate need of money would sell their organs. “The rich or reasonably well off,” the argument goes, “Don’t need the money so few of them would become donors under such a system.” Additionally, wealthy people could buy organs from the poor but the poor could not afford to buy organs if they needed them. Dr. Sally Satel is a Kidney transplant recipient and a resident scholar at the American Enterprise Institute in Washington D.C. She is editor of “When Altruism Isn’t Enough: The Case for Compensating Kidney Donors” (AEI Press, 2009) and a practicing psychiatrist and lecturer at the Yale University School of Medicine. She has long supported the idea of compensating organ donors. You can read the Wall Street Journal story here.
Dr. Sally Satel is a Kidney transplant recipient and a resident scholar at the American Enterprise Institute in Washington D.C. She is editor of “When Altruism Isn’t Enough: The Case for Compensating Kidney Donors” (AEI Press, 2009) and a practicing psychiatrist and lecturer at the Yale University School of Medicine. She has long supported the idea of compensating organ donors. You can read the Wall Street Journal story here. One idea is to provide lifetime health insurance, through Medicare or a private insurer for the donor. The donor would receive annual physicals, routine medical screening, and long-term follow-up, in addition to standard health coverage. A federally sponsored registry of donors could help physicians study long-term outcomes for donors and take steps to remedy physical or psychological difficulties that arise.
One idea is to provide lifetime health insurance, through Medicare or a private insurer for the donor. The donor would receive annual physicals, routine medical screening, and long-term follow-up, in addition to standard health coverage. A federally sponsored registry of donors could help physicians study long-term outcomes for donors and take steps to remedy physical or psychological difficulties that arise. The issue of paying for human organs is controversial to say the least but that does not mean it can’t or won’t work. Iran, which is usually not a good example for much of anything, allows for such a program and the result reportedly is that their waiting list has sharply declined and in some cases it has diminished entirely.
The issue of paying for human organs is controversial to say the least but that does not mean it can’t or won’t work. Iran, which is usually not a good example for much of anything, allows for such a program and the result reportedly is that their waiting list has sharply declined and in some cases it has diminished entirely. Everyone, unless you have the riches of Donald Trump, everyone complains about the cost of prescription drugs and the complaints are justified. No other country in the world pays as much for prescription drugs as Americans do. Big Pharma, that’s Washington DC talk for the huge pharmaceutical companies, is making sky high profits and they aren’t going to end anytime soon. In the latest year in which I was able to find numbers 2012 the top 11 global drug companies made nearly $85 billion in net profits. That’s net, folks, not gross. The gross number is, well, gross.
Everyone, unless you have the riches of Donald Trump, everyone complains about the cost of prescription drugs and the complaints are justified. No other country in the world pays as much for prescription drugs as Americans do. Big Pharma, that’s Washington DC talk for the huge pharmaceutical companies, is making sky high profits and they aren’t going to end anytime soon. In the latest year in which I was able to find numbers 2012 the top 11 global drug companies made nearly $85 billion in net profits. That’s net, folks, not gross. The gross number is, well, gross. mind. How do these people who are so obviously biased and in the industry’s pocket, get into these positions of power? I shouldn’t even ask the question, because the answer is so obvious. For example; PhRMA, (the Pharmaceutical Research and Manufacturers of America) which spent $18.4 million lobbying lawmakers last year and BIO (Bio-technology Innovation Organization) which spent $8.4 million, are among the most visible groups on Capitol Hill. Get this. Former Louisiana Congressman Billy Tauzin chaired the committee which oversees the drug industry. You know how he got the chairmanship? Well, he was a Democrat, but when the Republicans took over the majority he switched parties. Now that’s a lust for power. Then he abruptly resigned his congressional seat and shortly thereafter emerged as the new leader of PhRMA where was a paid a cool $2 million a year. That deal leaves a stench on the paper this is printed on.
mind. How do these people who are so obviously biased and in the industry’s pocket, get into these positions of power? I shouldn’t even ask the question, because the answer is so obvious. For example; PhRMA, (the Pharmaceutical Research and Manufacturers of America) which spent $18.4 million lobbying lawmakers last year and BIO (Bio-technology Innovation Organization) which spent $8.4 million, are among the most visible groups on Capitol Hill. Get this. Former Louisiana Congressman Billy Tauzin chaired the committee which oversees the drug industry. You know how he got the chairmanship? Well, he was a Democrat, but when the Republicans took over the majority he switched parties. Now that’s a lust for power. Then he abruptly resigned his congressional seat and shortly thereafter emerged as the new leader of PhRMA where was a paid a cool $2 million a year. That deal leaves a stench on the paper this is printed on. You probably didn’t know this but we, the United States and New Zealand are the only two countries in the world that allow prescription drug advertising. The companies are trying to put pressure on doctors to prescribe by going directly to consumers and asking them to ask their docs for a prescription of the latest snake oil and some of it is snake oil. Some drug companies will make minute changes in the chemical structure of a drug, rename it and call it a new drug. Prilosec, for example became Nexium. It was essentially the same drug but changing the formula a smidgeon and giving it a new name netted billions for the parent company.
You probably didn’t know this but we, the United States and New Zealand are the only two countries in the world that allow prescription drug advertising. The companies are trying to put pressure on doctors to prescribe by going directly to consumers and asking them to ask their docs for a prescription of the latest snake oil and some of it is snake oil. Some drug companies will make minute changes in the chemical structure of a drug, rename it and call it a new drug. Prilosec, for example became Nexium. It was essentially the same drug but changing the formula a smidgeon and giving it a new name netted billions for the parent company.  knows no bounds. Now I understand, many pharma companies are attempting to re-incorporate outside of the US in order to dodge U.S. taxes. Does that really surprise anyone?
knows no bounds. Now I understand, many pharma companies are attempting to re-incorporate outside of the US in order to dodge U.S. taxes. Does that really surprise anyone? Big pharma says paying physicians has little or no effect on what they prescribe. Ok, if that’s true why the drug do companies pay doctors all of that money if they aren’t getting a huge return on investment. To be fair, there are efforts to reduce the influence Pharma representatives have on physicians. Many hospitals and clinics no longer take samples as a display of independence, but that’s a double edged sword. A good any patients counted on getting those free samples to cut the cost of the drugs they take. Doctors claim these pharma payments have no effect on what they prescribe. But why would drug companies pay out all those millions of dollars if the practice didn’t provide them a healthy return on their investment?
Big pharma says paying physicians has little or no effect on what they prescribe. Ok, if that’s true why the drug do companies pay doctors all of that money if they aren’t getting a huge return on investment. To be fair, there are efforts to reduce the influence Pharma representatives have on physicians. Many hospitals and clinics no longer take samples as a display of independence, but that’s a double edged sword. A good any patients counted on getting those free samples to cut the cost of the drugs they take. Doctors claim these pharma payments have no effect on what they prescribe. But why would drug companies pay out all those millions of dollars if the practice didn’t provide them a healthy return on their investment? healthcare and big pharma pay their CEOs more than any other industry? Want proof? Median pay for healthcare and pharmaceutical executives amounted to $14.5 million in 2015, higher than for leaders in any other sector,
healthcare and big pharma pay their CEOs more than any other industry? Want proof? Median pay for healthcare and pharmaceutical executives amounted to $14.5 million in 2015, higher than for leaders in any other sector,  The population of the United States is about 320 million. Of that number 120,000 are on the national organ transplant waiting list. 22 of them die every day because there are not enough organs to go around. Numbers, just numbers. We hear them so often they are meaningless. But the numbers aren’t meaningless to the Husband who just lost his wife because there was no kidney for her, or the child who lost her dad because there was no liver. These numbers represent human lives, You or someone you love could be one of them some day and I know that from personal experience.
The population of the United States is about 320 million. Of that number 120,000 are on the national organ transplant waiting list. 22 of them die every day because there are not enough organs to go around. Numbers, just numbers. We hear them so often they are meaningless. But the numbers aren’t meaningless to the Husband who just lost his wife because there was no kidney for her, or the child who lost her dad because there was no liver. These numbers represent human lives, You or someone you love could be one of them some day and I know that from personal experience. transplant in South Africa. I remember telling one of my reporter colleagues that it was a really big deal because it would someday save thousands of lives. It never occurred to me that 40 years later I’d be one of those who benefited from Dr. Barnard’s pioneering efforts. I had a heart transplant In August of 2007
transplant in South Africa. I remember telling one of my reporter colleagues that it was a really big deal because it would someday save thousands of lives. It never occurred to me that 40 years later I’d be one of those who benefited from Dr. Barnard’s pioneering efforts. I had a heart transplant In August of 2007 The biggest problem we face, though, is procrastination. In case you don’t know what that is it is when you see that mess in your garage and say, I’ll get to that tomorrow, but tomorrow never comes. Polls and survey’s tell us that in excess of 90% of all Americans think organ donation is a great idea, but only about 40 percent actually become donors. And in some cases, not many, but some families will object to recovering the organs from a loved one for transplantation.
The biggest problem we face, though, is procrastination. In case you don’t know what that is it is when you see that mess in your garage and say, I’ll get to that tomorrow, but tomorrow never comes. Polls and survey’s tell us that in excess of 90% of all Americans think organ donation is a great idea, but only about 40 percent actually become donors. And in some cases, not many, but some families will object to recovering the organs from a loved one for transplantation. sitting. It only takes a few minutes, then tell your family, your physician and your spiritual or religious advisor…and you are done. You can formalize the process by adding “Organ donor” to your driver’s license, but again, be sure to tell your family what your wishes are so there’s no confusion when and if the time comes.
sitting. It only takes a few minutes, then tell your family, your physician and your spiritual or religious advisor…and you are done. You can formalize the process by adding “Organ donor” to your driver’s license, but again, be sure to tell your family what your wishes are so there’s no confusion when and if the time comes. So there is an urgency, both on your part and on the part of the recipient. Can you imagine what it feels like to be on a transplant list day after day, month after month, year after year, waiting for an organ, knowing you are dying and there’s little modern medicine can do short of a transplant. Think about that…seriously think about that for a minute.
So there is an urgency, both on your part and on the part of the recipient. Can you imagine what it feels like to be on a transplant list day after day, month after month, year after year, waiting for an organ, knowing you are dying and there’s little modern medicine can do short of a transplant. Think about that…seriously think about that for a minute. donation. So let’s take that on, too, while we are at it. Here’s’ what the American Transplant Foundation has to say about the subject:
donation. So let’s take that on, too, while we are at it. Here’s’ what the American Transplant Foundation has to say about the subject:


 remaining children Paul and Sara. Then on an otherwise happy day, Claire got the phone call no parent ever wants to receive. “Come to Sacramento right away,” said a hospital nurse who explained that Paul had suffered a massive stroke. He was found on the sidewalk by his house unconscious. It was estimated he had been there for three hours or more before he was discovered and now a web of wires and tubing connected him to the technology that kept his heart beating and his lungs working. Claire remembers that phone conversation as though it took place an hour ago, “When I got the call that my other son, Paul, was on life support and could I please come up to Sacramento to sign the necessary papers for his organ donations, I put the phone down and let out screams I didn’t know I had inside of me.”
remaining children Paul and Sara. Then on an otherwise happy day, Claire got the phone call no parent ever wants to receive. “Come to Sacramento right away,” said a hospital nurse who explained that Paul had suffered a massive stroke. He was found on the sidewalk by his house unconscious. It was estimated he had been there for three hours or more before he was discovered and now a web of wires and tubing connected him to the technology that kept his heart beating and his lungs working. Claire remembers that phone conversation as though it took place an hour ago, “When I got the call that my other son, Paul, was on life support and could I please come up to Sacramento to sign the necessary papers for his organ donations, I put the phone down and let out screams I didn’t know I had inside of me.” Procurement Organization and told that Paul’s driver’s license indicated he was an organ donor. Claire, also an organ donor, immediately agreed to honor Paul’s wishes. She was informed that he was in such good physical condition that all organs that were transplantable could be donated, but first they had to find recipients. That meant Paul would be kept on life support for several more days. Days in which Claire sat and stared at her immobilized son, tubes and wires still attached still breathing and warm to the touch of a mother’s hand.
Procurement Organization and told that Paul’s driver’s license indicated he was an organ donor. Claire, also an organ donor, immediately agreed to honor Paul’s wishes. She was informed that he was in such good physical condition that all organs that were transplantable could be donated, but first they had to find recipients. That meant Paul would be kept on life support for several more days. Days in which Claire sat and stared at her immobilized son, tubes and wires still attached still breathing and warm to the touch of a mother’s hand. us bereft, were it not for his generosity in wanting to be an organ donor at the end of his life, which we all hoped would be many years down the road, at least well after mine. The last thing he wanted was to be hooked up to any machine, but that is exactly what happened. We feel that because that was necessary to keep his organs going to fulfill his wish of organ donation, he would have approved being monitored by banks of machines, and being poked and prodded endlessly for three days in order for that to happen.
us bereft, were it not for his generosity in wanting to be an organ donor at the end of his life, which we all hoped would be many years down the road, at least well after mine. The last thing he wanted was to be hooked up to any machine, but that is exactly what happened. We feel that because that was necessary to keep his organs going to fulfill his wish of organ donation, he would have approved being monitored by banks of machines, and being poked and prodded endlessly for three days in order for that to happen. It is because of you and of course your loving son that I am alive. Please know that each time I feel my heart beat I think of your son. It is amazing to me that your son (my donor) and I have so much in common. I was blessed with receiving a new heart. I will never take that for granted. Please be assured that I am taking very good care of myself and that I am getting emotionally and physically stronger and stronger as each day passes. I look forward to meeting with you one day and am overwhelmed with the thought of that meeting.
It is because of you and of course your loving son that I am alive. Please know that each time I feel my heart beat I think of your son. It is amazing to me that your son (my donor) and I have so much in common. I was blessed with receiving a new heart. I will never take that for granted. Please be assured that I am taking very good care of myself and that I am getting emotionally and physically stronger and stronger as each day passes. I look forward to meeting with you one day and am overwhelmed with the thought of that meeting. agreed to an interview and to have me publish a blog. Here’s what she said.
agreed to an interview and to have me publish a blog. Here’s what she said. totally agree, and to go to the hospital every day to keep a vigil for the brain-dead body of their family member, while potential organ recipients are researched, measured, weighed, matched up, scrutinized and finally, all scheduled to be prepped for the exact same moment. While it was heart-wrenching to see my son for the last time as he was wheeled out of his room to the O.R. just down the hall for the recovery of his organs, it was so rewarding to hear directly from his heart recipient how much he appreciated the gift and to hear to what lengths he goes to protect it, to take care of it, to monitor it, to faithfully keep his checkup appointments, etc. I can only say it did this mother’s heart good to KNOW FOR SURE that Paul’s heart beats on, is appreciated, and cared for.
totally agree, and to go to the hospital every day to keep a vigil for the brain-dead body of their family member, while potential organ recipients are researched, measured, weighed, matched up, scrutinized and finally, all scheduled to be prepped for the exact same moment. While it was heart-wrenching to see my son for the last time as he was wheeled out of his room to the O.R. just down the hall for the recovery of his organs, it was so rewarding to hear directly from his heart recipient how much he appreciated the gift and to hear to what lengths he goes to protect it, to take care of it, to monitor it, to faithfully keep his checkup appointments, etc. I can only say it did this mother’s heart good to KNOW FOR SURE that Paul’s heart beats on, is appreciated, and cared for.

 doctor has prescribed an anti-depression medication for you like Remeron, Wellbutrin or Cymbalta. Chances are good, too, that if you‘ve been taking anti-depressants for a while you’ve found that after a while they seem to wear out so your doctor will prescribe a new one. There are scores of such medications out there so physicians have a huge variety from which to choose making it is easy to prescribe something different.
doctor has prescribed an anti-depression medication for you like Remeron, Wellbutrin or Cymbalta. Chances are good, too, that if you‘ve been taking anti-depressants for a while you’ve found that after a while they seem to wear out so your doctor will prescribe a new one. There are scores of such medications out there so physicians have a huge variety from which to choose making it is easy to prescribe something different.
 (ECT). Yes, ECT is sending electrical shocks into the brain, but it is not like the Shock Therapy of the old Boris Karloff movies or more recently, “One flew over the Cuckoos nest.” It is brief, painless, has few side effects and can be very effective. To the best of our knowledge most MDD therapies are covered by Medicare and other insurances, but check before you agree to be treated. It is not unusual for some patients to participate in all three forms of treatment.
(ECT). Yes, ECT is sending electrical shocks into the brain, but it is not like the Shock Therapy of the old Boris Karloff movies or more recently, “One flew over the Cuckoos nest.” It is brief, painless, has few side effects and can be very effective. To the best of our knowledge most MDD therapies are covered by Medicare and other insurances, but check before you agree to be treated. It is not unusual for some patients to participate in all three forms of treatment. Human communication and health are two topics I have been passionate about most of my life. So much so that I got three degrees in one and have spent most of my adult life digging deep into the other. Both are topics of such depth and expanse that no human being could come close to mastering the limitless scope of either. One facet that has especially fascinated me is the effect one has on the other, particularly, the impact that communication has on human health.
Human communication and health are two topics I have been passionate about most of my life. So much so that I got three degrees in one and have spent most of my adult life digging deep into the other. Both are topics of such depth and expanse that no human being could come close to mastering the limitless scope of either. One facet that has especially fascinated me is the effect one has on the other, particularly, the impact that communication has on human health. relationship can never be something one party feels and the other does not. It can be judged only in the eyes of both beholders. Just as you cannot make other people love you, you cannot make them feel good about the way you choose to communicate with them. Discovering how to meet the needs of someone else when you interact often requires a delicate dance until you match your own footsteps with theirs. But it is never as simple as that. There also has to be a meeting of minds and a link from the hearts. Reaching a level that makes for comfortable satisfying communication with people close to you can take years, even a lifetime. Sadly, if we don’t practice them with each interaction, we too easily forget the steps and we have to relearn them again and again.
relationship can never be something one party feels and the other does not. It can be judged only in the eyes of both beholders. Just as you cannot make other people love you, you cannot make them feel good about the way you choose to communicate with them. Discovering how to meet the needs of someone else when you interact often requires a delicate dance until you match your own footsteps with theirs. But it is never as simple as that. There also has to be a meeting of minds and a link from the hearts. Reaching a level that makes for comfortable satisfying communication with people close to you can take years, even a lifetime. Sadly, if we don’t practice them with each interaction, we too easily forget the steps and we have to relearn them again and again. No two human beings are alike. The needs they bring into a communication moment will never be the same. We’ve all known people we care about deeply who are so needy that it strains our powers to provide. Some spend their lives immersed in such insecurity and unexplained longing that you can never tell them often enough the affirmations they need to hear. No matter the number of times you praise some people, withhold it or disagree with them once, and you will have failed to meet their needs. Efforts to interact satisfactorily with those people can extract costs on the health of all parties concerned.
No two human beings are alike. The needs they bring into a communication moment will never be the same. We’ve all known people we care about deeply who are so needy that it strains our powers to provide. Some spend their lives immersed in such insecurity and unexplained longing that you can never tell them often enough the affirmations they need to hear. No matter the number of times you praise some people, withhold it or disagree with them once, and you will have failed to meet their needs. Efforts to interact satisfactorily with those people can extract costs on the health of all parties concerned. seems,” “Based on what I have read,” “Having dealt with this issue many times,” or simply, “My opinion on this issue is.” Declamations of certainty don’t invite open discussion. They don’t warmly welcome alternate views.
seems,” “Based on what I have read,” “Having dealt with this issue many times,” or simply, “My opinion on this issue is.” Declamations of certainty don’t invite open discussion. They don’t warmly welcome alternate views. deep inside every day. Few of us would deny the benefits to be derived from self study, self-improvement or the difficulty of sticking to this task. Even those of us who relish that challenge too often fail to see the need to do the same with others in our lives.
deep inside every day. Few of us would deny the benefits to be derived from self study, self-improvement or the difficulty of sticking to this task. Even those of us who relish that challenge too often fail to see the need to do the same with others in our lives. interpret when we listen. We cannot ignore these filters if we hope to function as and be perceived as sensitive communicators. Yes, we have our facial and body expressions to aid us when we interact face-to-face. Actually, non-verbal carries the bulk of the weight in effective listening: touching, nodding, laughing, leaning, smiling, tone, volume, pitch, pauses and countless other little things. Too many people believe they have mastered the art of sensitive listening. Yet, it is one of the most prized and least developed skills on earth.
interpret when we listen. We cannot ignore these filters if we hope to function as and be perceived as sensitive communicators. Yes, we have our facial and body expressions to aid us when we interact face-to-face. Actually, non-verbal carries the bulk of the weight in effective listening: touching, nodding, laughing, leaning, smiling, tone, volume, pitch, pauses and countless other little things. Too many people believe they have mastered the art of sensitive listening. Yet, it is one of the most prized and least developed skills on earth. Most important of all, when we write messages, we have to give careful consideration to the “tone” of the words we choose. Cocky and confident have similar meanings but are markedly different in tenor and tone. Connotations are built into countless words. In and of themselves, they can be negative, indifferent, condescending, hostile, or irreverent regardless of your intent. The possibilities are endless when it comes to the ways of skirting around saying someone is lying. We can refer to their stories, unsupported claims, or disingenuous declamations. My all-time favorite is “He is practiced in the artistry of shading the truth.”
Most important of all, when we write messages, we have to give careful consideration to the “tone” of the words we choose. Cocky and confident have similar meanings but are markedly different in tenor and tone. Connotations are built into countless words. In and of themselves, they can be negative, indifferent, condescending, hostile, or irreverent regardless of your intent. The possibilities are endless when it comes to the ways of skirting around saying someone is lying. We can refer to their stories, unsupported claims, or disingenuous declamations. My all-time favorite is “He is practiced in the artistry of shading the truth.” we have to earn every day with word and deed. None of the intimate communication problems I have identified here are simple to correct. The factors that contribute to each are complex and multi-faceted. It is too easy to create a new problem in our attempt to eliminate another. That doesn’t mean we stop trying. The first thing we have to remember is that none of our interactions have a distinct and separate beginning and end. Relationships exist on a continuum that cannot be taken out of context and treated as independent events.
we have to earn every day with word and deed. None of the intimate communication problems I have identified here are simple to correct. The factors that contribute to each are complex and multi-faceted. It is too easy to create a new problem in our attempt to eliminate another. That doesn’t mean we stop trying. The first thing we have to remember is that none of our interactions have a distinct and separate beginning and end. Relationships exist on a continuum that cannot be taken out of context and treated as independent events. An award winning high school speech and English teacher, Priscilla Diffie-Couch went on to get her ED.D. from Oklahoma State University, where she taught speech followed by two years with the faculty of communication at the University of Tulsa. In her consulting business later in Dallas, she designed and conducted seminars in organizational and group communication.
An award winning high school speech and English teacher, Priscilla Diffie-Couch went on to get her ED.D. from Oklahoma State University, where she taught speech followed by two years with the faculty of communication at the University of Tulsa. In her consulting business later in Dallas, she designed and conducted seminars in organizational and group communication.
 drunk. If it was a matter of choice, a matter of will power, a matter over which alcoholics had control they would not choose to live that way. It is a life of absolute misery, dishonesty and risk. Your best friend and worst enemy is the bottle, it totally controls your life. Every minute of your existence revolves around making sure you have access to alcohol. If you have to choose between eating and drinking, you’ll drink. If you have to choose between bleeding to death and drinking, you’ll choose bleeding and if you have to choose between those you love and alcohol, you will choose alcohol and all the while knowing it’s wrong — totally and absolutely wrong. Worse yet, as you continue to choose alcohol over what’s right, that cloud of oppressive guilt that follows you around will tighten its stranglehold forcing you to consume more in another feeble attempt to stop the agony.
drunk. If it was a matter of choice, a matter of will power, a matter over which alcoholics had control they would not choose to live that way. It is a life of absolute misery, dishonesty and risk. Your best friend and worst enemy is the bottle, it totally controls your life. Every minute of your existence revolves around making sure you have access to alcohol. If you have to choose between eating and drinking, you’ll drink. If you have to choose between bleeding to death and drinking, you’ll choose bleeding and if you have to choose between those you love and alcohol, you will choose alcohol and all the while knowing it’s wrong — totally and absolutely wrong. Worse yet, as you continue to choose alcohol over what’s right, that cloud of oppressive guilt that follows you around will tighten its stranglehold forcing you to consume more in another feeble attempt to stop the agony. I stopped to read the post and comments I mentioned earlier because I have an interest in the subject. Addiction runs in my family. I was a practicing alcoholic for a long time and the practice paid off, I became a perfect drunk. It started when I was a teen who thought a weekend of beer consumption was normal behavior. I realized at that early age that while others could have a can of beer or two and then quit, I couldn’t. I always drank until drunk (sometimes unconscious) or until we ran out of alcohol whichever came first.
I stopped to read the post and comments I mentioned earlier because I have an interest in the subject. Addiction runs in my family. I was a practicing alcoholic for a long time and the practice paid off, I became a perfect drunk. It started when I was a teen who thought a weekend of beer consumption was normal behavior. I realized at that early age that while others could have a can of beer or two and then quit, I couldn’t. I always drank until drunk (sometimes unconscious) or until we ran out of alcohol whichever came first. I’m sure there are many who have been heavy drinkers, made the decision to quit and did. Others counted on God’s intervention and it worked, but for the vast majority of alcoholism sufferers quitting is beyond their ability. That was and is e nature of my condition. I am absolutely convinced that my ability to quit drinking was unrelated to will power. An alcoholism counselor once told me, “If you think will power will work, the next time you have diarrhea, use will power to stop it.” Just the thought of drinking again scares the hell out of me.
I’m sure there are many who have been heavy drinkers, made the decision to quit and did. Others counted on God’s intervention and it worked, but for the vast majority of alcoholism sufferers quitting is beyond their ability. That was and is e nature of my condition. I am absolutely convinced that my ability to quit drinking was unrelated to will power. An alcoholism counselor once told me, “If you think will power will work, the next time you have diarrhea, use will power to stop it.” Just the thought of drinking again scares the hell out of me. Alcoholism is not only the failure to say “no” to the drug, it is also a complete abandonment of all that you know is right — a behavior change so great as to be unbelievable. The image of an alcoholic that many have is of a foul-smelling bum in dirty clothes who sleeps in a cardboard box in a dark, trash cluttered alley. He is inarticulate, uneducated and offensive. That’s the stereotype, but you know what? That’s only a partial picture.
Alcoholism is not only the failure to say “no” to the drug, it is also a complete abandonment of all that you know is right — a behavior change so great as to be unbelievable. The image of an alcoholic that many have is of a foul-smelling bum in dirty clothes who sleeps in a cardboard box in a dark, trash cluttered alley. He is inarticulate, uneducated and offensive. That’s the stereotype, but you know what? That’s only a partial picture. t closely had no idea that I had a secret life. They didn’t know that the double wide briefcase I carried was not full of office work. H, it carried a quart of vodka and a carton of cigarettes. They didn’t know that when I arrived at the office in in the morning, I had already had several drinks or that I had slept in a chair in the clothing I wore the day before. They were unaware that I hid my bottle in the bottom of the men’s room waste basket so whenever I wanted a drink, I just went to the men’s room. They didn’t know that behind the wall mirror in my bathroom at home, I had built a carefully hidden compartment to house my liquor supply. It was constructed while my wife was at work to ensure secrecy. The hidden latch on the wall mirror let it swing open to reveal several bottles sitting on a 2 X 4 shelf. It is where I got my first drink of the day, just a little something to get the hair off of my tongue and get my heart started. Neither friends nor family knew about the sandpit about six blocks from my home. It had a bottle of vodka hidden under the “No trespassing” sign that was only recoverable under the cover of night. There may have been other places as well and the bottles may still be there because I forgot where I put them.
t closely had no idea that I had a secret life. They didn’t know that the double wide briefcase I carried was not full of office work. H, it carried a quart of vodka and a carton of cigarettes. They didn’t know that when I arrived at the office in in the morning, I had already had several drinks or that I had slept in a chair in the clothing I wore the day before. They were unaware that I hid my bottle in the bottom of the men’s room waste basket so whenever I wanted a drink, I just went to the men’s room. They didn’t know that behind the wall mirror in my bathroom at home, I had built a carefully hidden compartment to house my liquor supply. It was constructed while my wife was at work to ensure secrecy. The hidden latch on the wall mirror let it swing open to reveal several bottles sitting on a 2 X 4 shelf. It is where I got my first drink of the day, just a little something to get the hair off of my tongue and get my heart started. Neither friends nor family knew about the sandpit about six blocks from my home. It had a bottle of vodka hidden under the “No trespassing” sign that was only recoverable under the cover of night. There may have been other places as well and the bottles may still be there because I forgot where I put them.
 vowed to go public with my addiction as a means to help me stay sober. Treatment, AA meetings, being public about my problem helped, I’ve not had a drink since a little before noon on that day in ’82.
vowed to go public with my addiction as a means to help me stay sober. Treatment, AA meetings, being public about my problem helped, I’ve not had a drink since a little before noon on that day in ’82.
 and how to determine if Medicare will pay for it. At some future date I might focus on other issues important to the disabled.
and how to determine if Medicare will pay for it. At some future date I might focus on other issues important to the disabled. Scooter or wheelchair? That’s probably not a
Scooter or wheelchair? That’s probably not a decision you will have to make, your physical condition may dictate what will work best for you, Disabled World offers this explanation. (
decision you will have to make, your physical condition may dictate what will work best for you, Disabled World offers this explanation. ( Let’s start with the most common question. “Will Medicare pay for my wheelchair or mobility scooter?” That single question is the cause of a lot of confusion, because the answer is, “Maybe.”
Let’s start with the most common question. “Will Medicare pay for my wheelchair or mobility scooter?” That single question is the cause of a lot of confusion, because the answer is, “Maybe.” (unpowered) wheelchair, a senior must have a condition which prevents them from moving around in their home as they go about daily living. Their disability cannot be resolved through the use of a cane or walker and the wheelchair cannot be necessary only for use outside the home.
(unpowered) wheelchair, a senior must have a condition which prevents them from moving around in their home as they go about daily living. Their disability cannot be resolved through the use of a cane or walker and the wheelchair cannot be necessary only for use outside the home.
 Recently I met a man my age who had a scooter identical to mine. I asked how he liked it and he told me that not only was it a great scooter but that Medicare had paid for it. Now I know better than that so I asked how that worked and he explained that with the help of his scooter supplier he found a physician who provided the medical certification he needed. Beware – if any supplier has a list of Doctors you can see who will approve your purchase it is likely you will get one fraudulently.
Recently I met a man my age who had a scooter identical to mine. I asked how he liked it and he told me that not only was it a great scooter but that Medicare had paid for it. Now I know better than that so I asked how that worked and he explained that with the help of his scooter supplier he found a physician who provided the medical certification he needed. Beware – if any supplier has a list of Doctors you can see who will approve your purchase it is likely you will get one fraudulently. pack it into the back of the mini-van how will you do that? Your scooter will have to be transportable, that means lightweight and easy to disassemble and assemble unless you can afford a power ramp on the back of your vehicle, one onto which you can drive so there’s no lifting or disassembling involved.
pack it into the back of the mini-van how will you do that? Your scooter will have to be transportable, that means lightweight and easy to disassemble and assemble unless you can afford a power ramp on the back of your vehicle, one onto which you can drive so there’s no lifting or disassembling involved. stands about 4 or 5 feet high from the back of your vehicle. It will help both drivers and pedestrians see you coming and add some safety insurance.
stands about 4 or 5 feet high from the back of your vehicle. It will help both drivers and pedestrians see you coming and add some safety insurance. Finally, this word. There have been admirable attempts at making the world more accessible, but they are too few and still too rare. In many buildings you will find stairways and no ramps. Disabled parking is often abused by those who don’t need it. Mobility carts in supermarkets and other businesses are wonderful, if you can get one. Again, too many people who don’t need them, ride them. Even the sidewalks can be problematic when cars parked in driveways overlap and block the sidewalk, forcing scooters and wheelchairs into the street. And, most importantly those of us who are disabled are simply not seen. I can’t tell you how many times people are looking over my head as they walk right into my scooter.
Finally, this word. There have been admirable attempts at making the world more accessible, but they are too few and still too rare. In many buildings you will find stairways and no ramps. Disabled parking is often abused by those who don’t need it. Mobility carts in supermarkets and other businesses are wonderful, if you can get one. Again, too many people who don’t need them, ride them. Even the sidewalks can be problematic when cars parked in driveways overlap and block the sidewalk, forcing scooters and wheelchairs into the street. And, most importantly those of us who are disabled are simply not seen. I can’t tell you how many times people are looking over my head as they walk right into my scooter. the way to the back of the elevator before anyone enters there is usually room for several more people and often they will stand back and allow me to do that. On other occasions, though, the crowd surges around me, packs the elevator and then as the door is closing they will look surprised when they see there is no room for me even though I was there first.
the way to the back of the elevator before anyone enters there is usually room for several more people and often they will stand back and allow me to do that. On other occasions, though, the crowd surges around me, packs the elevator and then as the door is closing they will look surprised when they see there is no room for me even though I was there first.“Strength does not come from physical capacity. It comes from an indomitable will.” – Mahatma Gandhi
Introduction by Bob Aronson
Dawn Anita Plumlee is family. I am proud to say she is not only a member of my personal family, but also my larger extended one, the Organ Donation family. She and her sister, Dr. Priscilla Diffic-Couch are frequent contributors here.
Dawn Anita has never had an organ transplant and likely won’t need one, nor has anyone in her immediate family, but she is as committed to our cause as any one of us who has either given or received a life-saving organ.
Dawn Anita and her husband Jerry have met adversity up close and personal, slapped it in the face, shoved it aside and forged ahead. They are two of the most positive people I know and share our passion for saving lives.
In a song, Kenny Rogers advised us to, “Know when to hold em, and Know when to fold em…” Dawn Anita knows and she ain’t likely to “Fold em” any time soon.
This inspirational story is true. Dawn Anita Credits her many successes to attitude and the power of positive thinking. This is her account of just one of those journeys.

The Power Of Positive Thinking
By Dawn Anita Plumlee
Lying in my hospital bed staring into the darkness while listening to the gloomy sounds that ring out in a hospital in the middle of the night…. buzzers beeping, patients calling for help and the sound of nurses’ footsteps scurrying down the hall, I was trying hard to wash the negative thoughts from my mind. I glanced over at my dear devoted husband Jerry sound asleep in the hospital chair beside my bed. His body was twisted, cram ped and confined. He looked very uncomfortable. I smiled when I saw that he hadn’t bothered to take off his cowboy boots. One toe was pointing to the ceiling and the other was pointing towards the wall. Soft, intermittent snoring sounds filled the air. Warm thoughts flooded my mind knowing he would go to the ends of the earth and back for me. I knew he was worried, and it was difficult for me to comprehend that I was here waiting for a blood transfusion. I closed my eyes and my thoughts drifted back in time to the events that had taken place over the past few months.
ped and confined. He looked very uncomfortable. I smiled when I saw that he hadn’t bothered to take off his cowboy boots. One toe was pointing to the ceiling and the other was pointing towards the wall. Soft, intermittent snoring sounds filled the air. Warm thoughts flooded my mind knowing he would go to the ends of the earth and back for me. I knew he was worried, and it was difficult for me to comprehend that I was here waiting for a blood transfusion. I closed my eyes and my thoughts drifted back in time to the events that had taken place over the past few months.
It was 2013. I turned 71 on my birthday, but in my heart I felt more like I was 51. Life had treated me good those 71 years,  I had a wonderful husband of 55 years, two beautiful children, seven terrific grandchildren, and three precious great-grandchildren. My health was excellent. I had never had any major illness and was not taking any kind of medication. I was retired and enjoyed the time I spent working on our small ranch, riding horses, taking care of cattle, and helping with the everyday chores that occur on a ranch. I was still active in music, writing songs, recording and singing and was preparing to enter the Miss Senior Oklahoma Pageant for the second time.
I had a wonderful husband of 55 years, two beautiful children, seven terrific grandchildren, and three precious great-grandchildren. My health was excellent. I had never had any major illness and was not taking any kind of medication. I was retired and enjoyed the time I spent working on our small ranch, riding horses, taking care of cattle, and helping with the everyday chores that occur on a ranch. I was still active in music, writing songs, recording and singing and was preparing to enter the Miss Senior Oklahoma Pageant for the second time.
I thought of all the hours Jerry and I had spent over the last few years clearing timber behind our house. The work was hard, dusty and dirty, and it seemed to be a never-ending chore, picking up stumps, trimming trees, and burning brush piles, driving the tractor disking and harrowing preparing the ground for planting grass. It was exhausting work and my energy level seemed to drain quickly, sometimes struggling to even catch my breath but never admitting to myself that anything was wrong.
My husband and I were taking our early morning walk when I suddenly stopped and exclaimed to him, “I can’t seem to walk and talk at the same time without running out of breath.” I thought to myself, “Boy, I have really let myself get out of shape,” so I began walking faster and longer. My stamina and ability to walk and talk without running out of breath did not seem to be improving.
Not wanting to admit anything could be wrong with my health, I dismissed the fact that I had suddenly dropped ten pounds, I experienced nausea nearly every day, my urine was a dark color, a nd I was constantly fatigued. My blood pressure regularly registered extremely low, and I knew something with my body wasn’t 100%, but I would not allow myself to be overly concerned. After all I was tough. I was a great believer in the power of positive thinking, so I was optimistic and believed strongly that I would be able to overcome any problems that I was having.
nd I was constantly fatigued. My blood pressure regularly registered extremely low, and I knew something with my body wasn’t 100%, but I would not allow myself to be overly concerned. After all I was tough. I was a great believer in the power of positive thinking, so I was optimistic and believed strongly that I would be able to overcome any problems that I was having.
I had chosen to perform an Elvis medley for my talent in the Miss Senior Oklahoma Pageant. The songs were upbeat, and it was my nature to put everything into each of my performances moving energetically on stage. During rehearsals I noticed I could not move as I normally did without becoming winded. I would have to bend over and breathe deeply in order to continue. The night of my actual performance, I gave it my all, but when I watched my performance on video, I was very disappointed. I knew I was subconsciously protecting myself during my performance in order to make it through the medley.
Dialing the phone, I felt weak and a wave of nausea hit me. Our daughter “Punkin” answered the phone and said anxiously, “What is it Mom?” I didn’t want to worry her. This was a very special occasion. Her daughter Rachel (our granddaughter) was getting married and the reception dinner was this evening. Fighting to hold back tears, I said, “Punkin, I’m not feeling very good, and I am so sorry, but Dad and I cannot make it to Rachel’s reception dinner, but we will definitely be at her wedding tomorrow.” Concerned, Punkin said, “Mom, are you okay?” Bravely, I replied, “Oh, I’m sure I’ll be fine by tomorrow. Tell Rachel we’re sorry, and we’ll see her at the wedding.”
My dad died at the age of 80 with congestive heart failure. Since I was experiencing shortness of breath, I was fearful that I might be having heart trouble, and I knew I had to find a primary care doctor. The first thing the doctor did was routinely complete blood work. They drew my blood on Tuesday. On Wed nesday I received a call from the doctor’s office saying they needed to draw some more blood. I went in on Thursday morning and gave some additional blood not really thinking much about it.
nesday I received a call from the doctor’s office saying they needed to draw some more blood. I went in on Thursday morning and gave some additional blood not really thinking much about it.
Late that afternoon I was helping my husband Jerry unload a truckload of sod to put on the lawn. Each time I grabbed a roll of sod and placed it on the lawn, I would have to bend over and catch my breath a minute before continuing. Pulling some sod off the truck, I noticed the farrier had arrived to shoe our horses. Jerry told me to go help him, and he would finish putting the sod on the lawn. Relieved, I happily went out to catch the horses for the farrier. I was surprised when I saw Jerry walking out to the barn motioning for me to come to him. He said, “Dawn Anita, the doctor’s office called five times and left word for you to call right away.” Knowing it was past 5:00, I said, “They’ll be closed now, I’ll call in the morning,” to which Jerry replied, “No, go call them now.”
Dialing the number, I thought to myself, “I wonder what they could possibly want?” As I had predicted, their office was closed, so I left a message. In less than thirty seconds the phone rang. It was the nurse from the doctor’s office. A little too urgently she said, “Mrs. Plumlee, you need to get to the emergency room  right away.” Confused, I asked, “What’s the problem?” to which she replied, “You have severe anemia and we have alerted ER that you are on your way.” I thought to myself, “Anemia, that doesn’t sound that urgent.” I asked, “Can’t this wait until tomorrow? Am I going to die tonight or what?” Jerry grabbed the phone and said, “Quit arguing with her, we’re going to the hospital right now.”
right away.” Confused, I asked, “What’s the problem?” to which she replied, “You have severe anemia and we have alerted ER that you are on your way.” I thought to myself, “Anemia, that doesn’t sound that urgent.” I asked, “Can’t this wait until tomorrow? Am I going to die tonight or what?” Jerry grabbed the phone and said, “Quit arguing with her, we’re going to the hospital right now.”
The waiting room at the ER was full when we arrived. Thinking I was in for a long wait, I walked to the front desk and gave them my name. The receptionist jumped up, motioned me through the door, quickly looked at my ID and medical cards and sent me back to a room. In less than five minutes, the doctor was there. Jokingly, I said, “Hey, Doc, my insurance must really pay good for you to get here so quick.” I realize now I was using humor to hide my fear of what was happening.
The doctor informed me that my hemoglobin count (HGB) was 5 .4, which was less than half of what it should be. That was a little alarming, but I didn’t realize just how serious it was. The doctor then asked “Mrs. Plumlee have you been bleeding anywhere?” and I responded, “Not that I’m aware of.” I guess he didn’t believe me, because he proceeded to perform a couple of rather unpleasant tests. A portable x-ray machine was wheeled into the room for x-rays of my chest, and the hospital ran several tests on my blood. The doctor ruled out cancer and indicated further testing would need to be done. I heard him say to the nurse “This might turn into a difficult case,” and he then told me he had ordered three units of blood. I was doing my best to be positive, but fear started creeping up my spine and my heart started beating faster; it felt like I couldn’t breathe.
.4, which was less than half of what it should be. That was a little alarming, but I didn’t realize just how serious it was. The doctor then asked “Mrs. Plumlee have you been bleeding anywhere?” and I responded, “Not that I’m aware of.” I guess he didn’t believe me, because he proceeded to perform a couple of rather unpleasant tests. A portable x-ray machine was wheeled into the room for x-rays of my chest, and the hospital ran several tests on my blood. The doctor ruled out cancer and indicated further testing would need to be done. I heard him say to the nurse “This might turn into a difficult case,” and he then told me he had ordered three units of blood. I was doing my best to be positive, but fear started creeping up my spine and my heart started beating faster; it felt like I couldn’t breathe.
And that’s how I ended up in the hospital waiting for a blood transfusion. My sister Priscilla called several times to see if they had given me the transfusion yet. I thought how nice it was of her to be so worried about me. I have to admit, I was more than a little worried myself, but if I had known what she knew, I would have been frantic. Most people with HGB as low as mine are not up and walking around. The organs begin to shut down, you’re a likely candidate for a heart attack, and it is not unusual for someone to lapse into a coma. Around 7:00 the next morning, the nurses changed shifts, and a new nurse came into my room. With a surprised look she said, “Oh, you’re awake.” I replied, “Oh yes, I’ve been awake most of the night,” not realizing that she had checked my stats before coming into my room, and she fully expected me to be in a coma.
Apparently the blood bank was having difficulty finding a match due to the antibodies in my blood. After 12 hours, I finally received three units. They tested it again after the transfusions, and my HGB had risen 4.2 points…thank goodness! My doctor came by before I was released, gave me some Prednisone and handed me a prescription. She told me that by tomorrow I should be feeling much better. She said she had referred my case to an oncologist/hematologist at the Cancer Center, and they would be calling me in a few days to set an appointment.
received three units. They tested it again after the transfusions, and my HGB had risen 4.2 points…thank goodness! My doctor came by before I was released, gave me some Prednisone and handed me a prescription. She told me that by tomorrow I should be feeling much better. She said she had referred my case to an oncologist/hematologist at the Cancer Center, and they would be calling me in a few days to set an appointment.
The next morning, I kept thinking, “The doctor said I should feel better today, but I have this strange sensation running through my veins.” I told Jerry I needed to lie down for a while. When I awoke, I heard voices in the kitchen and realized Jerry was talking to our son, Jerry Don. When I walked into the kitchen, tears were running down Jerry’s cheeks, and with a heavy voice, he said, “I thought I lost you because you always wake up when the phone rings, but you didn’t wake up, so I called Jerry Don.” I threw my arms around his neck and said, “I’m not going anywhere. I can beat this; I have lots of other things I need to do before I go anywhere.” He held me in his arms for a long time and softly whispered, “I love you more than you’ll ever know.”
 Walking into the Cancer Center, I glanced around at the people in the waiting room. There was one older gentleman sitting crumpled over in a wheel chair, a lady with no hair sitting on a couch, breathing through an oxygen tube, and a frail looking older couple sitting quietly holding hands. I thought to myself, “I don’t belong here; these people are really sick.” The nurse drew my blood and sent me to another room to see the doctor. After that visit, I was at the reception desk making another appointment when the doctor suddenly appeared holding a slip of paper.
Walking into the Cancer Center, I glanced around at the people in the waiting room. There was one older gentleman sitting crumpled over in a wheel chair, a lady with no hair sitting on a couch, breathing through an oxygen tube, and a frail looking older couple sitting quietly holding hands. I thought to myself, “I don’t belong here; these people are really sick.” The nurse drew my blood and sent me to another room to see the doctor. After that visit, I was at the reception desk making another appointment when the doctor suddenly appeared holding a slip of paper.
With a wide smile, he said, “Here are your results.” My HGB reading was 11.4, and I thought “Hallelujah!” I started jumping up and down clapping my hands with joy. Ever so gently the doctor reached out took my hand and hugged my neck.
My diagnosis was hemolytic anemia, and the hematologist was trying hard to determine what was causing the anemia. Over the next several months, he ran what I thought must have been every blood test that existed which included HIV and Hepatitis C and B. Every test was negative. He performed a bone marrow test, which also came back negative. Every time I went in for yet another test, I would experience small panic attacks. “What if my HGB has gone down; why can’t they find out what’s wrong?”
Since the blood tests revealed nothing that indicated the source of my anemia, my doctor ordered a CT scan of my chest. Picking up the results of the test to take to the pulmonologist, the words on the report jumped out at me, “Multiple findings in the chest  highly suspicious for atypical infection mainly mycobacterium avium complex (Mac Lung Disease) which can have an identical appearance as tuberculosis.” Deep inside I knew. I had Mac Lung Disease.
highly suspicious for atypical infection mainly mycobacterium avium complex (Mac Lung Disease) which can have an identical appearance as tuberculosis.” Deep inside I knew. I had Mac Lung Disease.
The pulmonologist did a bronchoscopy and washed my lungs out with saline. It would take several weeks for the cultures to grow before I would know the test results. The nurse called each time a test result was received, and so far they were all negative. When she called to say the doctor needed to see me, she didn’t have to tell me the results, I knew.
Sitting on the examination table waiting for the pulmonologist, I was trying my best to remain calm. The doctor’s voice seemed to be far off in the distance as he told me I had Mac Lung Disease. I felt like I was outside of myself listening to him, all the while thinking, “This can’t be happening to me.” He told me I needed to start taking 3 antibiotics a day for a period of 18 months; the m edication could affect my liver and kidneys, and two of them could cause color blindness and blurred vision. In a state of confusion, I asked, “How did I get this?”
edication could affect my liver and kidneys, and two of them could cause color blindness and blurred vision. In a state of confusion, I asked, “How did I get this?”
He replied, “You can get it from the ground, the water and the air,” and then it dawned on me…. all the hours I had spent picking up stumps, trimming trees, driving the tractor with no cab, being constantly exposed to all that dirt and dust. I had compromised my immune system and now I have this disease (MAC lung disease is not spread by person to person contact and is not considered to be contagious. It is a fairly rare disease with fewer than one person in 10,000 becoming sick from it).
I was not prepared to commit to taking the antibiotics. In a state of shock, I went home and started frantically searching the Internet for natural remedies. I tried quite a few of them over a period of several months. None of them worked. My hemoglobin dropped drastically again, and I went back to see the pulmonologist. With tears rolling down my cheeks, I could barely utter the words, “I’m afraid to take the antibiotics. Is there anything else I can do?” I could see the compassion in his eyes when he said, “I think I need to make you an appointment with an infectious disease doctor for a second opinion.”
The infectious disease doctor could not believe I had Mac Lung Disease. I had no symptoms associated with the disease, and he informed me that hemolytic anemia was not common with Mac Lung Disease. He stated he had HIV patients whose hemoglobin was not as low as mine. He thought they must have made a mistake on the reading, and he made the comment; “There is no way you could have been walking around with a reading that low. That would be like driving 100 miles in a car with no gas in the tank.” I told him my doctor and the hospital ran the test twice, and they both came up with the same results. He made the comment, “If I didn’t have your test results in front of me, I would not believe you have the disease.” For that reason, we decided to wait and see if I displayed any symptoms before starting the medication.
Once again, my hemoglobin plunged to an unsafe level. I spent many s leepless nights worrying about what I should do. If I didn’t take the antibiotics I could die, but if I did take them, I could be deathly ill for months from the effects of the medication or even lose my eyesight, and I would have no quality of life at all. Neither my hematologist nor my infectious disease doctor could definitely say that my anemia was caused from Mac Lung Disease, and they could not assure me that the antibiotics would cure my anemia.
leepless nights worrying about what I should do. If I didn’t take the antibiotics I could die, but if I did take them, I could be deathly ill for months from the effects of the medication or even lose my eyesight, and I would have no quality of life at all. Neither my hematologist nor my infectious disease doctor could definitely say that my anemia was caused from Mac Lung Disease, and they could not assure me that the antibiotics would cure my anemia.
I turned to my loved ones hoping they could help me make a decision. They were all concerned and wanted to help, but in the end, I knew it must be my decision. I thought about the terrible side effects of the antibiotics and the scary results reported by folks who had taken the antibiotics. Needless to say, I was apprehensive about how the medication would affect me. Finally, it came to me. Start thinking positive. After all, hope and positive thinking are the strongest medicines of all. I told myself I would not be one of the people who experienced any of the side effects, and I started taking the antibiotics. The infectious disease doctor prescribed two antibiotics to be taken twice daily for a period of two years. I have been taking them for 16 months. Within four months, my hemoglobin vastly improved without having to take Prednisone. I can’t know for sure what the future holds, whether my anemia will return when I stop the antibiotics, but I try to live my life to the fullest and fill every day with joy and laughter.
As I write this, I realize that my near death experience in no way compares to those of you who are struggling every day to overcome a serious illness such as cancer or heart disease or those of you who are on the transplant list waiting for a life-saving organ that can prolong your life. I bow my head to all of you brave people and recognize that the human spirit is strong and hope springs eternal. My thoughts and prayers go out to each of you, and if the words in my story brighten your day in some small way or inspire you to keep fighting and not give up hope, then I will have accomplished my mission in writing this story.
-0-
Editor’s note from Bob Aronson. Dawn Anita is my Wife Robin’s cousin. I have known her for about 15 years and she is an amazing woman. Not only is she one of America’s great country singers, her nearly boundless energy has benefited many. She has freely donated her time and talent to many worthwhile causes and is a longtime member of Organ Transplant Initiative and a frequent contributor to Bob’s Newheart Blogs.
All of us in the donation/transplantation community have benefited from her compassion and generosity. In 2013 she wrote, produced, directed and paid all costs for her Nashville, Tennessee recording of “The Gift Of Life.” She then donated the song to our Facebook group Organ Transplant Initiative to use as we see fit to promote organ donation. You can see the video here:
http://www.youtube.com/watch?v=eYFFJoHJwHs&feature=youtu.be
Dawn Anita’s story is inspirational because of her spirit. She just refuses to lose faith and to give in to adversity. As a performer she is the consummate professional. When she hits that very first note, Dawn Anita has captured the audience. I am proud to call her “Cousin” and friend. Thank you Dawn Anita and Jerry, you are wonderful examples of the American Spirit and of my favorite sentiment — “Never Give up.”







































































































































































































































































































You must be logged in to post a comment.